A mixed-reality rehearsal that prepares anxious patients for an MRI, and made them 100% more likely to call the experience engaging than standard prep videos.
MRI exams are routinely terminated when patients panic in the bore, and the population it hurts most is the one least able to cope with it.
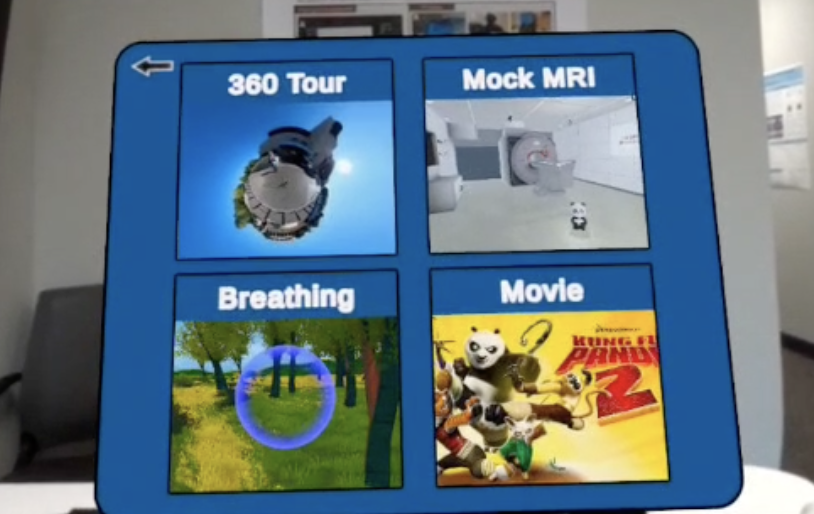
Standard prep is a passive video. The open question: could an interactive VR rehearsal on a standalone headset prepare patients better?
We ran a randomized crossover pilot (n=14) comparing a VR-MRI simulator against the standard hospital training video. Each participant experienced both, in counterbalanced order, rating engagement, preparedness, and how well each conveyed the real stressors of a scan.
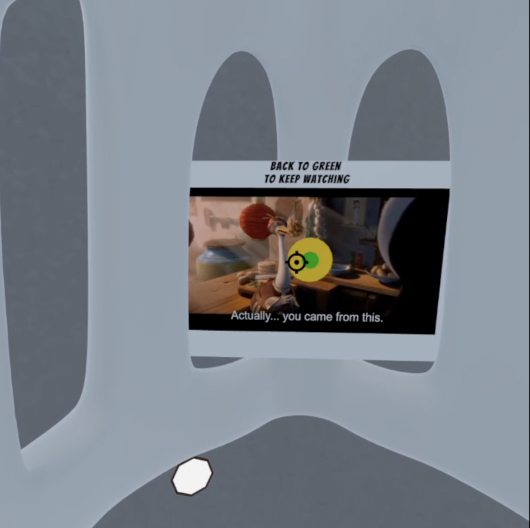
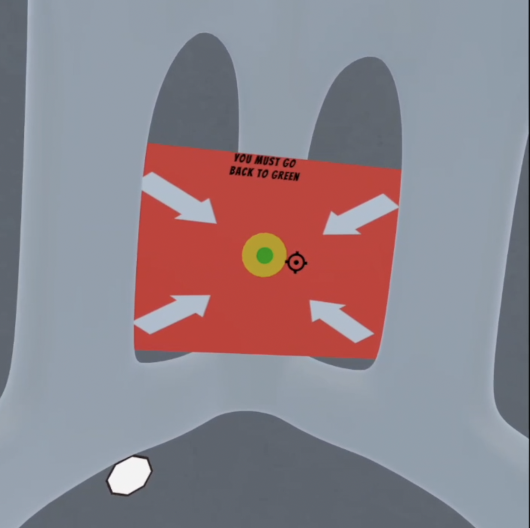
The design question wasn't "is VR cool." It was which medium teaches the two things that actually end scans: holding still, and the noise.
Authentic MRI noise (captured from real machines) plays in spatial audio to desensitize patients, and the Quest controller is rendered as the real-world emergency squeeze ball.
Deployed on Quest devices at Stanford Lucile Packard Children's Hospital and the Chariot Lab, with interest in future clinical studies.
I co-designed and developed the interaction and narrative flows (the breathing exercise, the 360° tour, the squeeze-ball input) and implemented the core mixed-reality functionality. I contributed to the study design for evaluating anxiety reduction, and helped translate clinical requirements into interaction constraints so the simulator stayed faithful to real MRI workflows while still feeling approachable.
Co-developed with Yue Yang; mentored by Prof. Bruce L. Daniel and Christoph Leuze (IMMERS), with clinical guidance from the Chariot Lab.
Average anxiety scores were lower with VR (1.14 vs 1.50) but not statistically significant (p = .317): almost certainly a floor effect from testing healthy volunteers with low baseline anxiety. The honest read: engagement and preparedness were the real, defensible wins, and the next study needs the actual anxious population the tool is built for. Designing the hold-still mechanic taught me that the hardest clinical instruction becomes learnable the moment you make the feedback immediate and the stakes playful.